|
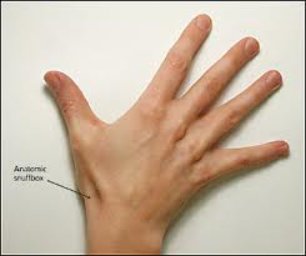
Scaphoid Fracture TreatmentThe types of scaphoid fracture treatment differ mainly due to the various stages of severity in which these injuries can present. What works for a non-displaced fracture may not work for a more severe, displaced or late-diagnosed injury. CASTING:Casting options for scaphoid fracture treatment must address the concept of reducing or eliminating unnecessary motion at the fracture site, because major tendon structures that operate the thumb and the index finger pass over the “anatomic snuff box” and can be responsible for considerable “micro-motion” at the site of the break; just enough to interfere with healing. Therefore, in many instances, casts must be applied that will restrict motion of the thumb, index finger and occasionally, the long finger.
Thumb Spica Cast
The thumb spica cast is considered to be the least effective casting option for any scaphoid injury beyond the “hairline” crack, non-displaced variety. This is mainly due to the fact that only the thumb is immobilized, and the motion caused by the use of the index and long fingers is not eliminated.
The cast, typically a short arm version that extends up the forearm to just below the elbow, incorporates the thumb, index and long fingers in their normal “position of function” (almost in a grasping position). It can be made of plaster or fiberglass.
One such device is called the Herbert or Herbert/Whipple screw. These screws are typically headless and constructed with threads of two different “pitches” or thread angles which, when screwed into place, help to compress the two fragments together for optimum healing. Surgical fixation is often accompanied by the use of some kind of bone graft substance, as there is the risk of post injury bone death due to avascular necrosis (loss of blood supply). Ideally, bone is taken (harvested) from a remote location on the patient, such as the hip crest. This tends to work better than fresh-frozen or synthetic alternatives, although there are many good ones out there today.
Leave Scaphoid Fracture Treatment; Go to Home Page
|

 What initially began decades ago as a simple insertion of a smooth pin to stabilize the scaphoid fracture components has evolved to various forms of fixation devices.
What initially began decades ago as a simple insertion of a smooth pin to stabilize the scaphoid fracture components has evolved to various forms of fixation devices. 

"We hope you enjoy your journey through Bone and Joint Pain.com"